
At the inaugural Integrated Care Action Summit (ICAS), Jodeme Goldhar led a Master Class in Collective Leadership for partners from all 58 Ontario Health Teams (OHTs) Participants included leaders from across health and social care sectors, industry partners and people with lived experience. The Masterclass explored what it takes to lead in complexity. The answer? Collective leadership. We know that the largest barriers to change, and also the greatest opportunities for transformation, are the deeper conditions of systems change - as outlined by the Collective Change Lab:
Paul Born, co-founder of the Tamarack Institute, emphasizes that collective leadership asks us to gather around a common agenda, to measure what matters, and to hold each other accountable with both grace and grit. It’s the art of turning shared hope into shared work.
Ways of working together that share the qualities of new radical containers that enable radical collaboration are essential to shifting these deeper conditions. This is about moving from old paradigms of authority to new models of collaboration, trust, and relational reciprocity. In integrated care, the concept of relational reciprocity is reflected in the pioneering work of Dr. Brenda Reiss-Brennan at Intermountain Healthcare. Her research shows that when teams operate with mutual respect, shared sense-making, and co-production with patients, outcomes improve at scale. Her work confirms what we see across systems worldwide: relationships are the infrastructure of transformation.
Traditional leadership assumes that answers come from the top. But in a system as complex as health care, no single leader, sector, or organization can solve the challenges we face. We need individual leadership that can work in distributed, relational, and regenerative ways. An approach to leadership that enables ecosystems to learn and adapt to achieve population-level outcomes.
This Masterclass explored “How do we lead forward next?” and “How might we pattern our next possible future given how we are ripe to own the path ahead, to lead together individually and together?” This means shifting from teaching leaders to designing ecosystems that learn. When purpose, trust, reflection and feedback are present, leadership becomes a collective regenerative force for transformation to take root and endure.
This reflects what scholars like Peter Senge, Otto Scharmer, and Margaret Wheatley have long pointed to: leadership is no longer an individual act, but a systems act. Their work invites us to move beyond developing “leaders” and instead shape ecosystems that learn, adapt, and regenerate.
In order to ensure collective action as the path, we must shift:
These shifts echo what global change leaders like Dr. Helen Bevan have long championed: large-scale transformation happens when power is redistributed, agency is expanded, and people are mobilized through networks, not hierarchies. Bevan’s work on New Power, social movement thinking, and large-scale change aligns deeply with this moment in integrated care.
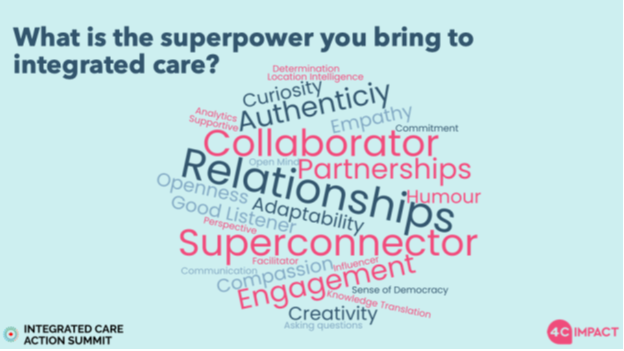
The Masterclass reminded us that insight without action is only half the story. Commitments, both individual and collective, are what transform ideas into real outcomes for population health. And in that room, you could feel those commitments taking shape. Leaders weren’t just talking about change; they were owning it, together. When asked about their unique superpowers to advance integrated care, responses like “connecting people,” “curiosity,” and “openness” filled the room, proof that the strength of this work lies in our collective leadership.
As we move forward, the challenge is to keep this momentum alive: to lean into collaboration, nurture creativity, and embrace the shared responsibility of building a healthier, more integrated future for all Ontarians. The summit was a recommitment, the real impact will come from the actions we take now, as one team, united by shared purpose and driven by patterning our possible future.
This blog is Part 2/2 of our series on the 2025 Integrated Care Action Summit and was co-created by Jodeme Goldhar, Samantha Laxton and Meghan Perrin.
Read Part 1: Accelerating Integrated Care: Harnessing Our Collective Potential: A Keynote Designed to Ignite Collective Action here